Living with diabetes means paying close attention to things that others might easily ignore. A tiny pebble in your shoe, a tight strap, or a minor scratch can turn into a serious medical issue if you have high blood sugar. This happens because diabetes can damage your nerves (causing a loss of feeling) and narrow your blood vessels (reducing healing blood flow).
When a wound or ulcer forms on a diabetic foot, doctors do not just look at it and guess the treatment. They use specific, internationally recognised systems to assess exactly how bad the wound is. This process is called grading diabetic foot ulcers.
By categorising the wound, your healthcare team can speak a common language, decide how aggressively to treat it, and predict the chances of saving the foot. In this deep-dive guide, we will break down the most popular classification systems, from the classic Wagner scale to the detailed University of Texas system, explaining what each grade means in plain English.
What Does “Grading Diabetic Foot” Mean?
Grading diabetic foot refers to the medical process of assessing and scoring a diabetic foot ulcer based on its severity.
Doctors look at how deep the wound is, whether there is an active infection, and if there is a lack of blood flow (ischaemia). Grading an existing ulcer is different from overall diabetic foot risk grading, which assesses a person’s chances of developing an ulcer in the future. Proper grading instantly tells the medical team whether a patient needs simple dressings, strong antibiotics, or urgent surgery to prevent an amputation.
Why Grading Diabetic Foot Matters
You might wonder why doctors spend time assigning numbers and letters to a wound instead of just treating it immediately.
Grading diabetic foot is the cornerstone of effective care. Firstly, it creates a roadmap for treatment planning. A superficial scratch needs a very different approach compared to a deep wound touching the bone.
Secondly, it dictates referral urgency. A high grade tells a local clinic that the patient must be rushed to a hospital with a vascular surgeon. It also helps doctors predict the healing time and the amputation risk. Finally, consistent grading allows for clear documentation, so if you see a different doctor next week, they know exactly if your foot is getting better or worse.
Diabetic Foot Grading vs Diabetic Foot Risk Classification
These two terms sound similar, but they happen at entirely different stages of a patient’s journey.
Diabetic foot grading is used when a patient already has an open wound or ulcer. The systems used here (like Wagner or Texas) measure the physical damage present in that specific hole in the skin.
Diabetic foot risk classification, on the other hand, is for prevention. It is used when the skin is completely intact. Doctors check your nerves, pulses, and foot shape to stratify your risk of getting an ulcer in the future. One deals with the current disaster, while the other tries to predict and stop future ones.
Basic Clinical Features Doctors Assess Before Grading
Before a doctor assigns a score or grade to your foot, they perform a thorough physical examination. They are looking for specific warning signs.
They check the ulcer depth to see if it stops at the skin or goes down to the fat, muscle, tendon, or bone. They look for signs of bacterial infection, such as redness, warmth, pus, and foul smells.
They also assess for ischaemia (poor blood flow) by feeling the pulses in your feet and checking if the skin is cold or pale. They test for neuropathy (nerve damage) using a small plastic thread to see if you can feel pressure. Finally, they check for foot deformity and any signs of black, dead tissue, known as gangrene.
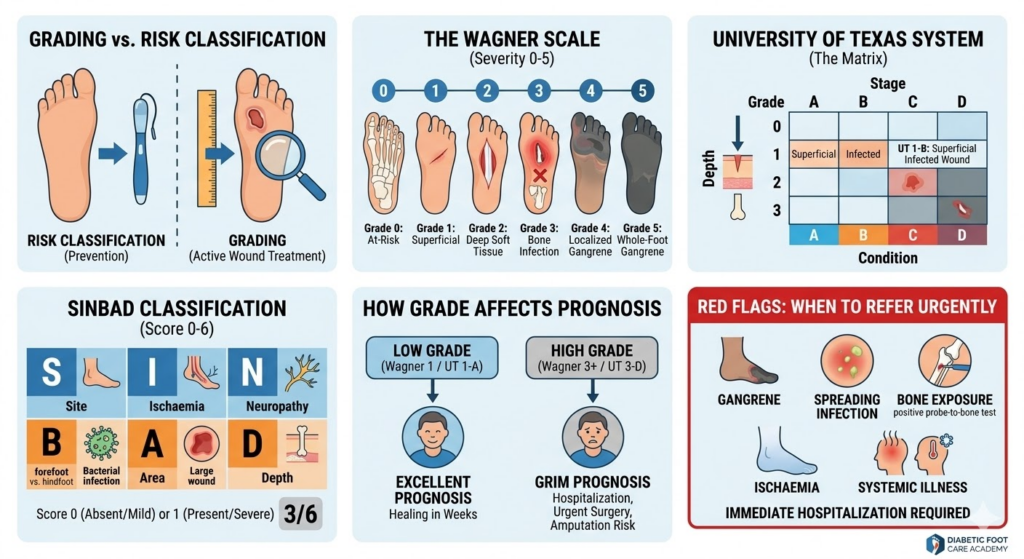
Wagner Diabetic Foot Ulcer Grading System
The Wagner-Meggitt classification is the oldest and most widely recognised system for grading diabetic foot ulcers.
Developed in the 1970s, it remains popular in clinics across India and the world because it is incredibly simple to use and easy to remember. It runs on a scale from 0 to 5.
The Wagner system mainly measures two things: the physical depth of the wound and the presence of tissue death (gangrene). While it is highly practical, its main drawback is that it does not clearly separate infection and ischaemia in the early stages, grouping them all together as the wound deepens.
Wagner Grade 0
This is the starting point. In Wagner Grade 0, there is no open ulcer on the foot. The skin is completely intact.
However, it is considered a “high-risk foot.” The patient might have severe nerve damage, thick calluses, or a foot deformity (like a Charcot foot or bunions). These deformities change how the person walks, putting high pressure on specific spots. It is a pre-ulcerative stage that requires good footwear and regular podiatry care to stop the skin from breaking open.
Wagner Grade 1
When the skin finally breaks, it becomes a Wagner Grade 1 ulcer.
This is a superficial wound. It has destroyed the top layers of the skin (the epidermis and dermis) but it does not go any deeper. It has not reached the underlying fat or muscle tissue. There is usually no major infection at this stage. With prompt offloading (taking the weight off the foot) and proper dressings, a Grade 1 ulcer has a very high chance of healing quickly.
Wagner Grade 2
In Wagner Grade 2, the ulcer has become significantly deeper.
The wound has punched through the skin and the fat, reaching down into the deeper soft tissues. You might be able to see the tendon, ligament, or joint capsule at the base of the wound.
Even though the wound is deep and looks frightening, a strict Grade 2 classification means there is no deep abscess (collection of pus) and no osteomyelitis (infection of the bone). It requires aggressive wound care and close monitoring to prevent the bone from getting infected.
Wagner Grade 3
This is where the situation becomes a serious medical emergency.
A Wagner Grade 3 ulcer is a deep wound that is now severely infected. The infection has spread deep into the foot, creating an abscess, or causing joint sepsis. Most critically, this grade usually involves osteomyelitis, meaning the bacteria have started eating into the bone itself.
Patients with a Grade 3 ulcer almost always require hospital admission, intravenous (IV) antibiotics, and surgical procedures to clean out the infected tissue and dead bone.
Wagner Grade 4
Wagner Grade 4 moves beyond just an open, infected wound into the territory of tissue death.
This grade indicates localised gangrene. Gangrene happens when the blood supply to a specific part of the foot is completely cut off, causing the tissue to turn black and die.
In Grade 4, the gangrene is restricted to a specific area, usually the toes, the forefoot, or the heel. Treatment often involves amputating the dead portion (like removing a toe) to save the rest of the foot, alongside procedures to open up blocked blood vessels.
Wagner Grade 5
This is the most severe and devastating stage in the Wagner classification.
Wagner Grade 5 indicates extensive gangrene that involves the whole foot. The tissue death has spread so far that the foot can no longer be saved. The lack of blood supply and the massive infection pose a direct threat to the patient’s life.
At this stage, the only medical option is a major amputation, usually below or above the knee, to stop the deadly infection from spreading into the rest of the body.
University of Texas Diabetic Foot Classification System
While the Wagner system is easy, many modern doctors prefer the University of Texas (UT) Diabetic Foot Classification System.
The UT system was created because Wagner had a blind spot: a superficial wound could be highly infected or have zero blood flow, completely changing how dangerous it is.
The UT system adds much more detail. It uses a matrix, like a grid. It measures the physical depth of the wound (using Grades) and perfectly pairs it with the presence of infection and ischaemia (using Stages). This makes it a far more accurate tool for predicting if an amputation will be needed.
University of Texas Grades and Stages
To use the UT system, the doctor must assign both a Number (the Grade) and a Letter (the Stage) to the ulcer.
The Grades range from 0 to 3, purely focusing on how deep the hole is. The Stages range from A to D, focusing entirely on what is complicating the wound (infection or poor blood flow).
By combining them, a doctor can give a highly specific diagnosis, such as “Grade 1, Stage C,” which instantly paints a clear clinical picture of the patient’s foot.
University of Texas Grade 0
Just like the Wagner system, Grade 0 means there is no current, active ulcer.
It covers pre-ulcerative lesions, completely healed ulcers that have scarred over, or a foot that is severely at risk due to bony deformities. The skin remains closed, but the foot requires protective footwear and daily inspection.
University of Texas Grade 1
A UT Grade 1 is a superficial wound.
It involves the top layers of the skin but does not penetrate down into the deeper structures. It does not involve any tendon, capsule, or bone. It is a shallow, surface-level break in the skin barrier.
University of Texas Grade 2
A UT Grade 2 wound is deep.
The ulcer has eaten through the skin and the subcutaneous fat. At the bottom of the wound, the doctor can physically see or probe a tendon or a joint capsule. However, the wound does not go deep enough to touch the actual bone.
University of Texas Grade 3
This is the deepest wound category in the UT system.
A Grade 3 wound penetrates completely through the soft tissue, directly exposing the bone or the inner joint space. When a doctor gently inserts a sterile metal probe into the ulcer, they can feel it hit hard bone (this is known as a positive probe-to-bone test).
University of Texas Stages A to D
Once the depth (Grade) is assigned, the doctor adds the Stage to describe the complications.
- Stage A: The wound is clean. There is no infection and no ischaemia (blood flow is good).
- Stage B: The wound is infected. It has bacteria, pus, or spreading redness, but blood flow is still okay.
- Stage C: The wound is ischaemic. The blood supply is extremely poor, making healing almost impossible, but there is no active infection.
- Stage D: The worst-case scenario. The wound is both heavily infected AND ischaemic. The foot has no blood flow to fight the aggressive bacteria.
A “Grade 3, Stage D” ulcer has a very high probability of ending in amputation.
SINBAD Classification for Diabetic Foot Ulcers
Another highly effective system used by specialists is the SINBAD classification.
SINBAD is an acronym that makes it easy for nurses and doctors to remember the six critical features of a diabetic ulcer: Site, Ischaemia, Neuropathy, Bacterial infection, Area, and Depth.
Each of these six categories is scored as either 0 (absent/mild) or 1 (present/severe). The total score ranges from 0 to 6. A higher score means a worse prognosis. SINBAD is incredibly useful for clinical communication between different hospital departments and for national medical audits.
IWGDF Approach to Diabetic Foot Ulcer Classification
The International Working Group on the Diabetic Foot (IWGDF) sets global standards for diabetes care.
The IWGDF stresses why validated systems matter. They strongly advise against doctors just writing “bad ulcer” in a patient’s file. Instead, they recommend using validated systems like SINBAD or the WIfI (Wound, Ischemia, foot Infection) classification.
The IWGDF insists that clinicians should routinely include assessments of perfusion (blood flow), extent of tissue loss, and infection severity for every single patient, ensuring no critical warning signs are missed.
NICE Diabetic Foot Risk Grading (Risk Stratification, Not Ulcer Grade)
The UK’s National Institute for Health and Care Excellence (NICE) guidelines focus heavily on stopping the ulcer before it even starts.
This is a risk stratification system, not an ulcer grading system. It is used during routine annual diabetic check-ups when the feet are currently intact. It divides patients into four clear pathways: Low risk, Moderate risk, High risk, and Active diabetic foot problem.
Low-Risk Diabetic Foot
A patient has a low-risk diabetic foot if they have completely normal sensation and good blood circulation.
They can feel the testing monofilament on their toes, and the doctor can easily feel strong pulses on the top of their feet. They have no major risk factors except perhaps some mild callus buildup. These patients usually just need their standard annual foot check and basic advice on moisturizing and wearing comfortable shoes.
Moderate-Risk Diabetic Foot
A moderate-risk foot means the first signs of trouble have appeared.
The patient has either developed neuropathy (they cannot feel the monofilament test, meaning their protective pain sensation is gone) OR they have peripheral arterial disease (weak pulses and poor blood flow) OR they have a foot deformity.
Because one of the protective mechanisms of the foot is compromised, these patients need to see a foot care specialist every 3 to 6 months.
High-Risk Diabetic Foot
A high-risk foot is in extreme danger of breaking down.
These patients have multiple risk factors combined (like neuropathy AND poor blood flow). They may also fall into this category if they are on renal replacement therapy (dialysis), or if they have a history of a previous foot ulcer or a previous amputation.
They require intense, frequent monitoring from a specialist diabetic foot team, often every 1 to 2 months, along with custom-made orthopaedic footwear.
Active Diabetic Foot Problem
This category is for patients facing an immediate crisis.
An active diabetic foot problem means the patient currently has an open ulcer, a spreading infection (cellulitis), gangrene, or an unexplained hot, red, swollen foot (which is the hallmark of an acute Charcot foot fracture).
Patients in this category bypass routine clinics and require immediate, urgent referral to a multidisciplinary diabetic foot team or hospital casualty department.
Wagner vs University of Texas vs SINBAD – Which Grading System Is Better?
There is ongoing debate in the medical community about which system is superior.
For simple comparison, Wagner is the easiest to use quickly, but it lacks detail. It ignores ischaemia entirely until the foot turns black.
The University of Texas system is much better because its inclusion of infection and ischaemia provides a highly accurate prediction of whether the wound will heal or lead to an amputation. SINBAD is less about detailed surgical planning and more about tracking outcomes and performing global audits. Most specialists agree that Texas or SINBAD are clinically superior to Wagner.
Which Diabetic Foot Grading System Is Most Common in Practice?
Despite its flaws, the Wagner classification remains arguably the most common system used globally, especially in general practice and smaller clinics in India.
Its simplicity means any doctor or nurse can use it without needing a chart. However, specialised diabetic foot clinics and vascular surgeons are increasingly shifting towards the Texas or WIfI systems. They recognise that knowing a wound’s depth is useless if you do not also document whether the foot has enough blood supply to heal that depth.
How Diabetic Foot Grading Affects Treatment
The grade assigned to your foot directly dictates your medical treatment plan.
For a superficial Grade 1 ulcer, the treatment involves simple dressings and offloading (using a special boot or cast to take weight off the foot).
If the grading shows infection (like UT Stage B or Wagner 3), aggressive oral or IV antibiotics are immediately started. If the grading highlights ischaemia, a vascular assessment is triggered to see if stents or bypass surgery are needed to restore blood flow. High grades almost always mean hospital admission and surgical cleaning (debridement).
How Diabetic Foot Grading Affects Prognosis
Prognosis simply means the predicted outcome of the disease.
Grading is the best crystal ball doctors have. A low-grade, clean ulcer with good blood flow has an excellent prognosis; healing time might just be a few weeks.
Conversely, a high-grade ulcer (like UT Grade 3, Stage D) comes with a grim prognosis. It predicts prolonged hospitalisation, a very high rate of recurrence, and severely diminished limb salvage chances, meaning a major amputation is highly probable.
Common Mistakes in Grading Diabetic Foot
Healthcare providers must be meticulous to avoid dangerous grading errors.
A massive mistake is ignoring ischaemia. A doctor might grade a wound as purely superficial, failing to realise that without blood flow, that shallow wound will never close.
Another error is missing deep infection severity. A wound might look small on the surface, but a massive pocket of pus could be hiding near the bone. Using only depth to grade the wound, while failing to document neuropathy or pedal pulses, leads to incomplete care and tragic outcomes.
When to Refer Urgently Based on Diabetic Foot Grade
General practitioners must know when a foot is beyond standard clinic care.
Urgent, same-day referral to an emergency department or specialised foot clinic is required if the patient exhibits any signs of gangrene (black tissue), spreading deep infection, or suspected osteomyelitis (bone infection).
Critical ischaemia (a pale, freezing cold, painful foot) or signs of systemic illness (where the foot infection causes a high fever, rapid heart rate, and confusion) are massive red flags requiring immediate hospitalisation to save the patient’s life and limb.
Real-Life Scenario
Mr. Gupta, a 62-year-old shopkeeper with poorly controlled Type 2 diabetes, noticed a small, painless blister on the bottom of his big toe. Because he had neuropathy (numbness), it did not hurt, so he ignored it.
Two weeks later, the blister opened into a deep hole, and his toe became red and swollen. He visited his local doctor, who properly assessed the wound. The doctor probed the wound and felt the bone. He also noted a foul-smelling pus discharge, though Mr. Gupta’s foot pulses were strong.
Using the University of Texas system, the doctor graded it as a Grade 3, Stage B ulcer (bone deep, with infection, but no ischaemia). Recognising the high risk of bone infection (osteomyelitis), the doctor urgently referred him to a diabetic foot clinic. Mr. Gupta was admitted, given IV antibiotics, and had a minor surgery to clean the infected bone. Because the doctor graded the foot accurately and acted fast, Mr. Gupta’s toe was saved.
Expert Contribution
Dr. Anjali Mehta, a senior vascular and endovascular surgeon, explains the vital role of these systems:
“In our diabetic foot clinics, the most heartbreaking cases are the ones that arrive too late because a superficial-looking wound was underestimated. Grading a diabetic foot is not just academic paperwork; it is a life-saving triage tool. I always tell junior doctors: do not just look at the hole in the foot. Look at the whole foot. Is it warm? Is there a pulse? Using a comprehensive system like the University of Texas classification forces you to assess the blood supply and the infection, which are the true killers of the diabetic limb.”
Recommendations Grounded in Proven Research and Facts
The global approach to managing diabetic foot complications is strictly evidence-based.
According to the International Working Group on the Diabetic Foot (IWGDF) guidelines, clinicians must use a validated classification system (like SINBAD, Texas, or WIfI) to standardise communication and audit outcomes.
Furthermore, the American Diabetes Association (ADA) strongly recommends that all patients with diabetes undergo a comprehensive foot evaluation at least annually to identify risk factors for ulcers and amputations. Research consistently proves that early risk stratification and aggressive grading of active ulcers reduce major lower-limb amputation rates by up to 50%.
Frequently Asked Questions on Grading Diabetic Foot
What are the 5 stages of diabetic foot?
When using the popular Wagner grading system, diabetic foot ulcers are classified into stages from 0 to 5. Grade 0 is intact skin at risk. Grade 1 is a superficial ulcer. Grade 2 is a deep ulcer reaching tendons. Grade 3 involves deep bone infection or an abscess. Grade 4 is localised gangrene (tissue death), and Grade 5 is whole-foot gangrene.
How to grade diabetic foot?
To grade a diabetic foot, a doctor will first physically examine the wound. They will measure how deep it goes (skin, fat, or bone). They will check for signs of infection (pus, redness) and test for poor blood flow (feeling for pulses). Based on these findings, they map the symptoms onto a standard chart, like the Wagner or University of Texas classification system.
What is the Wagner scoring system?
The Wagner scoring system is a 0 to 5 scale used by doctors to assess the severity of a diabetic foot ulcer. It focuses primarily on how deep the wound is and whether dead tissue (gangrene) is present. While simple to use, it is less detailed than newer systems because it does not separately score blood flow issues.
What is the triad of DFU?
The triad of a Diabetic Foot Ulcer (DFU) refers to the three major underlying medical problems that combine to cause severe foot damage. These are Neuropathy (nerve damage causing loss of feeling), Ischaemia (poor blood circulation), and Infection (bacterial invasion of the wound). All three must be managed to heal the foot.