
When most people think about diabetes, they immediately picture type 1 or type 2. But there is a lesser-known form called type 3c diabetes, also known as pancreatogenic diabetes, that develops when the pancreas is damaged by disease rather than by autoimmune attack or insulin resistance. If you or a loved one has been diagnosed with this condition, one of the first questions that likely comes to mind is: what does this mean for life expectancy?
The answer is complex and depends heavily on the underlying cause of the pancreatic damage, how well the diabetes is managed, and whether complications develop. Type 3c diabetes is not just a sugar problem; it is a sign that the pancreas has suffered significant injury, and that underlying damage often carries its own risks beyond the diabetes itself. Understanding these risks, knowing what factors influence survival, and learning how to optimise your management can make a meaningful difference in both how long and how well you live.
This comprehensive guide examines what current research tells us about type 3c diabetes life expectancy. We will explore how this condition affects survival compared with other diabetes types, what specific risk factors shorten or extend life, how treatment choices impact outcomes, and what steps you can take to improve your prognosis. Whether you are newly diagnosed or have been living with type 3c diabetes for years, this evidence-based overview will help you understand your situation and work effectively with your healthcare team.
What Is Type 3c Diabetes and Why Does It Affect Life Expectancy?
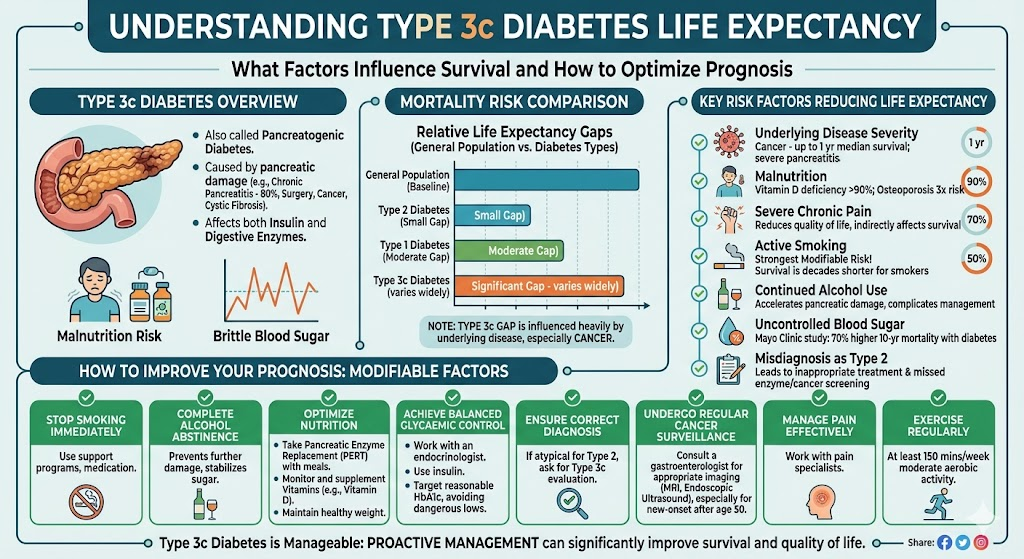
Type 3c diabetes mellitus, also called pancreatogenic diabetes, is a form of secondary diabetes that occurs when disease or injury damages the pancreas. Unlike type 1 diabetes, where the immune system attacks insulin-producing cells, or type 2 diabetes, where the body becomes resistant to insulin, type 3c diabetes results from physical destruction of pancreatic tissue. This damage affects not only the insulin-producing islet cells but often the enzyme-producing exocrine tissue as well.
The most common cause of type 3c diabetes is chronic pancreatitis, accounting for nearly 80% of cases. Other causes include acute pancreatitis, pancreatic cancer, cystic fibrosis, hemochromatosis, and pancreatic surgery. Because the underlying pancreatic disease continues to progress independently of the diabetes, patients with type 3c diabetes face risks from both conditions simultaneously.
This dual burden explains why type 3c diabetes life expectancy differs from that of type 1 or type 2 diabetes. While all forms of diabetes carry increased mortality risk from cardiovascular disease, kidney failure, and other complications, type 3c diabetes adds the risks of the underlying pancreatic condition. Chronic pancreatitis can lead to malnutrition, severe pain, pancreatic cancer, and liver disease. Pancreatic cancer, when present, has a five-year survival rate of less than 10%. Even without cancer, the ongoing inflammation and fibrosis of chronic pancreatitis creates a state of physiological stress that affects multiple organ systems.
Research published in the Journal of Clinical Medicine found that patients with type 3c diabetes have a significantly worse prognosis than those with type 2 diabetes. Compared with type 2 diabetic patients, those with type 3c diabetes have higher risks of pancreatic cancer, hypoglycaemia, microvascular and macrovascular complications, and all-cause mortality.
. This finding was reinforced by a nationwide study from New Zealand that followed over 10,000 patients, showing that post-pancreatitis diabetes mellitus was associated with a 13% higher risk of all-cause mortality compared with type 2 diabetes.
How Rare Is Type 3c Diabetes and Why Does Misdiagnosis Matter?
Type 3c diabetes is far more common than most people realise, yet it remains frequently misdiagnosed. Population studies suggest that 5% to 10% of all diabetes cases in Western populations are actually type 3c diabetes, making it the second most common form of diabetes in adults after type 2
. In some populations with high rates of chronic pancreatitis, the prevalence may be even higher.
Despite this prevalence, research from Germany found that only about half of type 3c diabetes cases are correctly classified. Most are misdiagnosed as type 2 diabetes because physicians fail to consider pancreatic disease as an underlying cause.
. This misdiagnosis matters enormously for life expectancy because it leads to inappropriate treatment. Patients with type 3c diabetes often have poor glycaemic control compared with type 2 diabetic patients, require insulin earlier, and have different nutritional needs due to exocrine pancreatic insufficiency.
When type 3c diabetes is misclassified as type 2, patients may be prescribed metformin or other oral agents that are poorly tolerated or ineffective. They may not receive pancreatic enzyme replacement therapy, leading to malnutrition and vitamin deficiencies. They may not be screened appropriately for pancreatic cancer. All of these factors can worsen outcomes and reduce life expectancy.
Comparing Life Expectancy: Type 3c vs Type 1 and Type 2 Diabetes
Understanding where type 3c diabetes stands in comparison to other diabetes types helps frame realistic expectations and highlights why aggressive management is so important.
Mortality Risk Compared with Type 2 Diabetes
Multiple large-scale studies have consistently shown that type 3c diabetes carries higher mortality risk than type 2 diabetes. The New Zealand nationwide cohort study found that post-pancreatitis diabetes mellitus had a 13% higher risk of all-cause mortality compared with age- and sex-matched type 2 diabetic patients
. This increased risk was driven particularly by higher rates of cancer death, infectious disease mortality, and gastrointestinal disease mortality.
A more detailed analysis published in Diabetologia broke down mortality risks by cause and demographics. Researchers found that women with post-pancreatitis diabetes had a 1.8 times higher risk of cancer mortality compared with women with type 2 diabetes, while men showed no significant difference in cancer death rates. Both men and women with post-pancreatitis diabetes had significantly higher risks of death from non-vascular, non-cancer causes, which includes infections, gastrointestinal diseases, and other complications.
The study also revealed important age-related differences. Younger adults with post-pancreatitis diabetes showed the greatest life expectancy gaps compared with both type 1 and type 2 diabetic patients. Those under 45 years of age had a 2.9 times higher risk of all-cause mortality compared with type 2 diabetes, and a 2.1 times higher risk compared with type 1 diabetes. These gaps narrowed with advancing age but remained significant even in older adults
.
Comparison with Type 1 Diabetes
When compared with type 1 diabetes, type 3c diabetes still shows worse outcomes in many studies. The Diabetologia analysis found that both men and women with post-pancreatitis diabetes had lower life expectancy up to age 64 compared with type 1 diabetic patients
. This may seem surprising given that type 1 diabetes is often diagnosed in childhood and carries risks of severe hypoglycaemia and diabetic ketoacidosis. However, modern management of type 1 diabetes has dramatically improved survival, while type 3c diabetes often occurs in the context of ongoing pancreatic disease, malnutrition, and pain that complicate management.
Life Expectancy in Specific Populations
For patients with fibrocalculous pancreatic diabetes, a form of tropical chronic pancreatitis common in certain regions, long-term survival data shows improvement over past decades. A cohort study of 370 patients found that about 80% were alive 35 years after their first episode of abdominal pain, with a median survival of 25 years after diabetes diagnosis. However, these figures remain considerably lower than the age- and sex-matched general population, with diabetic nephropathy being the main cause of death
In chronic pancreatitis patients undergoing surgery, ten-year survival was just 63.5% in a large study, highlighting the need for careful monitoring after surgical intervention
. Smokers with chronic pancreatitis had particularly poor outcomes, with mortality rates around 80% after 20 years compared with 30 years for non-smokers
What Factors Influence Life Expectancy in Type 3c Diabetes?
Several key factors determine how type 3c diabetes affects individual life expectancy. Understanding these can help patients and doctors target interventions where they will have the most impact.
Underlying Pancreatic Disease Severity
The severity and progression of the underlying pancreatic disease is perhaps the strongest predictor of survival. Chronic pancreatitis that continues to progress with frequent flare-ups, increasing calcification, or development of complications like pseudocysts carries worse prognosis than stable, well-managed disease. Pancreatic cancer as the underlying cause dramatically reduces life expectancy, with most patients surviving less than one year after diagnosis
Glycaemic Control Quality
While type 3c diabetes is notoriously difficult to control due to its “brittle” nature with frequent hypoglycaemic and hyperglycaemic swings, achieving reasonable glycaemic control remains important for longevity. A study from the Mayo Clinic found that chronic pancreatitis patients who developed diabetes had a 70% higher risk of ten-year mortality compared with those who did not develop diabetes, suggesting that the diabetic state itself adds significant risk
.
However, the target for glycaemic control in type 3c diabetes may differ from other forms. Because these patients lack the normal glucagon response to hypoglycaemia and may have unpredictable food absorption due to exocrine insufficiency, overly aggressive blood sugar control can lead to dangerous low blood sugar episodes. Guidelines suggest keeping blood glucose slightly above normal to improve quality of life and avoid hypoglycaemia, while still preventing the long-term complications of hyperglycaemia.
Nutritional Status and Malabsorption
Malnutrition is a major factor affecting survival in type 3c diabetes. The combination of exocrine pancreatic insufficiency, poor appetite due to pain and nausea, and increased metabolic demands from chronic inflammation leads to weight loss and nutrient deficiencies. Low body weight and body mass index are consistently associated with poor quality of life and likely contribute to reduced survival.
Vitamin D deficiency affects over 90% of chronic pancreatitis patients and is associated with poor glycaemic control and bone disease. Osteoporosis occurs in about 34% of these patients, three times the rate in the general population, increasing fracture risk
. Proper nutritional support, including pancreatic enzyme replacement and vitamin supplementation, is essential for improving outcomes.
Pain Control and Quality of Life
Severe abdominal pain is the dominant symptom in chronic pancreatitis and profoundly affects quality of life. Studies using the SF-36 quality of life questionnaire show that pain severity correlates with deterioration in all physical and mental health domains
. Poor quality of life is associated with unemployment, social isolation, and depression, all of which can indirectly affect survival through reduced self-care capacity and healthcare engagement.
Smoking and Alcohol Use
Smoking is one of the most important modifiable risk factors affecting life expectancy in type 3c diabetes. The long-term survival study of chronic pancreatitis patients found that smokers had mortality rates of around 80% after 20 years, compared with 30 years for non-smokers
. Smoking accelerates pancreatic damage, increases cancer risk, and worsens cardiovascular outcomes. Alcohol abstinence is similarly crucial, as continued drinking accelerates pancreatitis progression and complicates diabetes management.
Cancer Risk and Surveillance
Type 3c diabetes is a risk factor for pancreatic cancer, and conversely, pancreatic cancer can present as new-onset diabetes. Research from the Spanish National Cancer Research Centre confirmed that a high percentage of type 3c diabetes cases are caused by underlying pancreatic cancer, which should prompt early diagnostic interventions
. Both chronic pancreatitis and diabetes are independent risk factors for pancreatic malignancy, and their combination creates a particularly high-risk state. Regular surveillance for cancer, though challenging given the deep location of the pancreas, is an important component of management.
Real-Life Scenario: Navigating Type 3c Diabetes Prognosis
Mr. Patel, a 52-year-old man with a fifteen-year history of alcohol-related chronic pancreatitis, was referred to an endocrinology clinic after his general practitioner noted worsening blood sugar control. He had been diagnosed with type 2 diabetes five years earlier and was taking metformin, but his HbA1c remained elevated at 8.5%. He reported significant weight loss, foul-smelling stools, and frequent abdominal pain.
Further investigation revealed that Mr. Patel actually had type 3c diabetes. His pancreatic imaging showed extensive calcification, and his pancreatic enzyme levels were very low. He was started on pancreatic enzyme replacement therapy, which improved his digestion and weight. His diabetes medication was switched to insulin, which provided better glycaemic control than metformin, which he had poorly tolerated due to gastrointestinal side effects.
Over the next three years, Mr. Patel stopped drinking alcohol completely and quit smoking with support from a cessation programme. He maintained reasonable glucose control with HbA1c around 7.5%, though he experienced occasional hypoglycaemic episodes that required dose adjustments. He developed diabetic retinopathy requiring laser treatment, but his kidney function remained stable.
Now, at age 58, Mr. Patel continues to work part-time. While his life expectancy is likely reduced compared with the general population due to his pancreatic disease and diabetes, his proactive management of nutrition, glucose control, and lifestyle factors has given him the best possible outcome. His case illustrates that while type 3c diabetes carries inherent risks, attentive management can significantly improve both survival and quality of life.
Expert Contribution: A Gastroenterologist’s Perspective on Longevity
Dr. Sarah Chen, a consultant gastroenterologist specialising in pancreatic disorders, shares her insights on type 3c diabetes life expectancy: “The most important message I give my patients is that type 3c diabetes is manageable, and the underlying pancreatic disease, not the diabetes itself, usually determines survival. I have patients who have lived twenty-five years or more with this condition because they took control of the factors they could influence.”
Dr. Chen emphasises the importance of correct diagnosis: “I see too many patients who were treated for years as type 2 diabetics when they actually had pancreatic disease driving their diabetes. They were on the wrong medications, not getting enzyme replacement, and not being screened for pancreatic cancer. Correcting the diagnosis immediately changes their trajectory.”
She also stresses lifestyle modification: “Stopping smoking and alcohol is non-negotiable. These are the single most important factors that patients can control. I also push aggressively for nutritional support. Many of these patients are malnourished, and proper enzyme replacement with meals, vitamin D supplementation, and maintaining healthy weight can dramatically improve their resilience.”
Regarding cancer surveillance, Dr. Chen notes: “We do not have perfect screening tools for pancreatic cancer, but in high-risk patients, particularly those with new-onset diabetes after age 50 or those with strong family history, we use MRI and endoscopic ultrasound to look for early tumours. Catching pancreatic cancer early is one of the few ways to significantly extend life expectancy in this population.”
Recommendations Grounded in Proven Research and Facts
Based on current evidence, here are key recommendations for improving life expectancy and quality of life in type 3c diabetes:
Ensure correct diagnosis and classification. If you have diabetes and gastrointestinal symptoms, pancreatic disease history, or atypical features for type 2 diabetes, ask your doctor to evaluate for type 3c diabetes. Proper classification leads to appropriate treatment.
Stop smoking immediately. Smoking is the strongest modifiable risk factor for reduced survival in chronic pancreatitis. Smoking cessation programmes, nicotine replacement, and medications like varenicline can help. The survival difference between smokers and non-smokers is measured in decades.
Maintain complete alcohol abstinence. Alcohol accelerates pancreatic damage and interferes with diabetes management. Even moderate drinking is harmful in this population. Alcohol also causes unpredictable blood sugar fluctuations and increases hypoglycaemia risk.
Optimise nutritional status. Take pancreatic enzyme replacement therapy with every meal and snack if prescribed. Ensure adequate protein intake. Monitor and supplement fat-soluble vitamins, particularly vitamin D. Maintain healthy body weight; being underweight is associated with poor outcomes.
Achieve reasonable glycaemic control without excessive hypoglycaemia. Work with your diabetes team to set appropriate HbA1c targets, usually slightly less aggressive than for type 1 or type 2 diabetes to avoid dangerous lows. Insulin is often necessary and should be managed with careful monitoring.
Manage pain effectively. Uncontrolled pain reduces quality of life and affects survival through multiple pathways. Work with a pain specialist if needed. Options include medications, nerve blocks, and in selected cases, surgery.
Undergo appropriate cancer surveillance. Discuss with your gastroenterologist whether you need regular imaging to screen for pancreatic cancer, particularly if you have new-onset diabetes after age 50, strong family history, or other risk factors.
Exercise regularly. Guidelines recommend at least 150 minutes of moderate aerobic exercise per week for type 3c diabetes patients. Exercise improves insulin sensitivity, cardiovascular health, and quality of life, though insulin doses may need adjustment to prevent hypoglycaemia.
Key Takeaways: Understanding Type 3c Diabetes Life Expectancy
First, type 3c diabetes life expectancy is generally reduced compared with both the general population and patients with type 1 or type 2 diabetes, primarily due to the underlying pancreatic disease rather than the diabetes itself.
Second, the degree of reduction in life expectancy varies enormously based on the cause of the pancreatic damage, with pancreatic cancer carrying the worst prognosis and chronic pancreatitis allowing for many years of survival with proper management.
Third, younger patients with type 3c diabetes show the greatest survival gaps compared with other diabetes types, highlighting the importance of early, aggressive intervention in this population.
Fourth, modifiable risk factors, particularly smoking and alcohol use, have profound impacts on survival that exceed those seen in many other chronic diseases. Smoking cessation can add years to life expectancy.
Fifth, correct diagnosis is essential because misclassification as type 2 diabetes leads to inappropriate treatment, poor glycaemic control, and missed opportunities for nutritional support and cancer surveillance.
Sixth, while type 3c diabetes cannot be reversed, it can be managed effectively with insulin therapy, pancreatic enzyme replacement, nutritional optimisation, and lifestyle modification to improve both survival and quality of life.
Finally, patients should work with multidisciplinary teams including gastroenterologists, endocrinologists, nutritionists, and pain specialists to address the complex needs of this condition.
Frequently Asked Questions on Type 3c Diabetes Life Expectancy
What should a type 3c diabetic eat?
Type 3c diabetic patients should eat a diet rich in soluble fibre and low in fat, with adequate protein to prevent malnutrition. Small, frequent meals help stabilise blood sugar. Since many patients have exocrine pancreatic insufficiency, pancreatic enzyme replacement therapy is essential with meals to ensure nutrient absorption. Fat-soluble vitamins, especially vitamin D, should be supplemented. Avoid large portions and space meals throughout the day to prevent blood sugar spikes.
How rare is type 3c diabetes?
Type 3c diabetes is not rare; it affects 5% to 10% of all diabetic patients in Western populations, making it the second most common form of diabetes in adults after type 2. However, it is frequently misdiagnosed as type 2 diabetes, with studies showing only about half of cases are correctly classified. Chronic pancreatitis is the underlying cause in nearly 80% of cases
.
Can type 3c diabetes be reversed?
No, type 3c diabetes cannot be reversed because it results from permanent damage to pancreatic tissue and islet cells. Unlike type 2 diabetes where insulin resistance can improve with weight loss and lifestyle changes, type 3c diabetes involves structural destruction of the pancreas that cannot be regenerated. However, the condition can be effectively managed with insulin therapy, enzyme replacement, and lifestyle modifications to improve quality of life and survival.
Can you drink alcohol with type 3c diabetes?
No, alcohol should be completely avoided in type 3c diabetes. Alcohol accelerates the progression of chronic pancreatitis, worsens pancreatic inflammation and fibrosis, and complicates diabetes management. Alcohol also acutely inhibits glucose production by the liver and can cause dangerous hypoglycaemia, especially in patients taking insulin. Abstinence from alcohol is essential for improving outcomes.
Is type 3c diabetes dangerous?
Yes, type 3c diabetes can be dangerous if not properly managed. It carries higher mortality risk than type 1 or type 2 diabetes due to the underlying pancreatic disease. Risks include severe hypoglycaemia from absent glucagon response, malnutrition from exocrine insufficiency, pancreatic cancer, and cardiovascular complications. However, with proper management including insulin therapy, enzyme replacement, and lifestyle modifications, these risks can be significantly reduced.
What are the symptoms of type 3c diabetes?
Symptoms include typical diabetes symptoms such as increased thirst, frequent urination, fatigue, and blurred vision, plus symptoms related to pancreatic disease. These may include abdominal pain, weight loss, greasy or foul-smelling stools (steatorrhoea) from fat malabsorption, and digestive problems. Many patients also experience severe pain from chronic pancreatitis. The combination of diabetes symptoms with gastrointestinal complaints should prompt evaluation for type 3c diabetes.
How is type 3c diabetes treated?
Treatment includes insulin therapy, which is often required because oral medications are frequently ineffective or poorly tolerated. Pancreatic enzyme replacement therapy is essential for addressing exocrine insufficiency and malabsorption. Nutritional support with vitamin supplementation, particularly vitamin D, is important. Lifestyle modifications including smoking cessation, alcohol abstinence, and regular exercise are crucial. Pain management and cancer surveillance may also be necessary.
What is the life expectancy for someone with type 3c diabetes?
Life expectancy in type 3c diabetes varies widely depending on the underlying cause. For chronic pancreatitis-related diabetes, median survival after diagnosis is around 25 years, though this is improving with modern management. Younger patients have greater survival gaps compared with other diabetes types. Smoking dramatically reduces life expectancy, with smokers showing 80% mortality after 20 years versus 30 years for non-smokers. Pancreatic cancer as the underlying cause carries the worst prognosis. Proper management can significantly improve survival.
References:
- PMC – Glycemic Variability in Pancreatogenic Diabetes Mellitus https://pmc.ncbi.nlm.nih.gov/articles/PMC11423834/
- Nature – Risk of cardiovascular disease and mortality in patients with diabetes and acute pancreatitis history https://www.nature.com/articles/s41598-022-21852-7
- PMC – Risk of cause-specific death and life expectancy in post-pancreatitis diabetes mellitus https://pmc.ncbi.nlm.nih.gov/articles/PMC9254257/
- PubMed – Fibrocalculous pancreatic diabetes long-term survival analysis https://pubmed.ncbi.nlm.nih.gov/8908394/
- ScienceDirect – Survival Rates and Cause of Death in Chronic Pancreatitis https://www.sciencedirect.com/science/article/abs/pii/S1091255X23077363
- Diabetes Journals – Mortality and Glycemic Control in Chronic Pancreatitis With and Without Diabetes https://diabetesjournals.org/diabetes/article/72/Supplement_1/1324-P/150752/1324-P
- PMC – Increased risk of type 3c diabetes mellitus after acute pancreatitis https://pmc.ncbi.nlm.nih.gov/articles/PMC9749482/
- Wiley – Post-pancreatitis diabetes mellitus is common in chronic pancreatitis https://onlinelibrary.wiley.com/doi/full/10.1002/ueg2.12344
- Gastroenterology Advisor – Prior Acute Pancreatitis Indicates Risk for Diabetes, Mortality https://www.gastroenterologyadvisor.com/news/prior-acute-pancreatitis-risk-for-diabetes-mortality/
- Sage Journals – Diabetes mellitus secondary to pancreatic diseases (type 3c) https://journals.sagepub.com/doi/10.1177/1479164118764062
- FACS – Largest Study on Long-Term Follow-Up of Chronic Pancreatitis Patients https://www.facs.org/media-center/press-releases/2023/largest-study-on-long-term-follow-up-of-chronic-pancreatitis-patients-highlights-need-for-closer-monitoring-after-surgery/
- PMC – Diagnosis and treatment of diabetes mellitus in chronic pancreatitis https://pmc.ncbi.nlm.nih.gov/articles/PMC3831209/
- Mission Cure – Type 3c Diabetes (Pancreatogenic Diabetes) https://mission-cure.org/complications-of-chronic-pancreatitis/type-3c-diabetes/
- MDPI – Pancreatogenic Type 3C Diabetes https://www.mdpi.com/2392-7674/5/2/40
- CNIO – Diabetes type 3c is confirmed as an early manifestation of pancreatic cancer https://www.cnio.es/en/news/publications/diabetes-type-3c-early-manifestation-pancreatic-cancer/
- PMC – Management of pancreatogenic diabetes https://pmc.ncbi.nlm.nih.gov/articles/PMC5003514/
- PMC – Assessment of quality of life in patients with chronic pancreatitis https://pmc.ncbi.nlm.nih.gov/articles/PMC3539476/
- PMC – Quality of life in chronic pancreatitis https://pmc.ncbi.nlm.nih.gov/articles/PMC4088129/


