
When we think about diabetes complications, we usually picture problems with the eyes, kidneys, or feet. But there is another major organ that often suffers in silence: the bladder.
For millions of people living with diabetes, frequent washroom trips or difficulty passing urine become a frustrating part of daily life. Many dismiss these issues as a normal sign of getting older. However, these symptoms often point to a specific medical condition known as diabetic cystopathy.
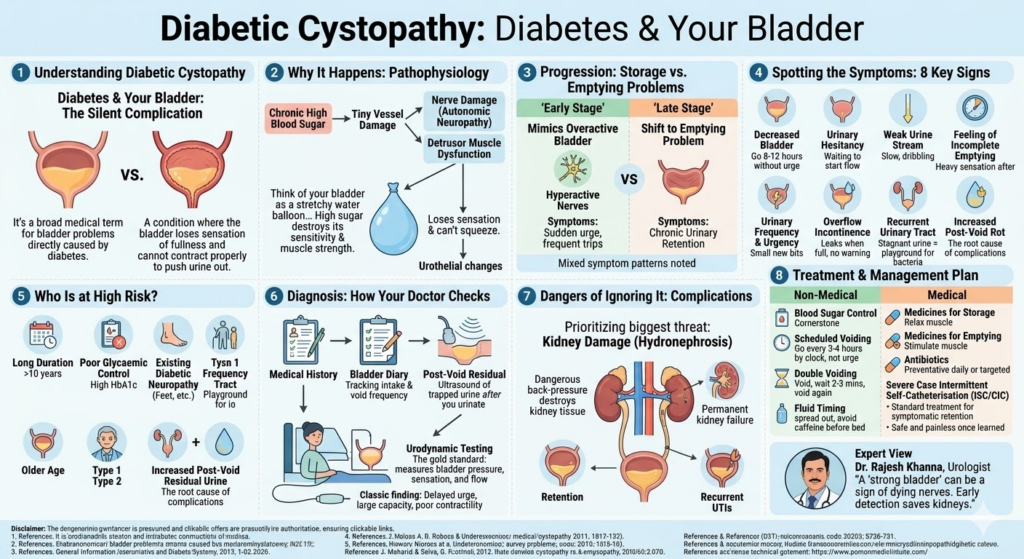
Diabetic cystopathy is a common but frequently overlooked complication of chronic high blood sugar. It fundamentally changes how your bladder feels, stores, and empties urine. If left untreated, it can lead to severe infections and even permanent kidney damage.
In this comprehensive guide, we will explore everything you need to know about diabetic cystopathy. We will break down why it happens, how to spot the early warning signs, and the best medical and lifestyle treatments available today to help you regain control of your bladder health.
What Is Diabetic Cystopathy?
Diabetic cystopathy is a broad medical term used to describe a range of bladder problems directly caused by diabetes mellitus.
It is officially classified as a type of diabetic bladder dysfunction. To put it simply, it is a condition where the bladder loses its ability to sense when it is full and struggles to contract properly to push urine out.
This condition is intimately linked to diabetic autonomic neuropathy. The autonomic nervous system controls the automatic, involuntary functions of our body, like our heartbeat, digestion, and bladder control. When diabetes damages these specific nerves, the brain and the bladder stop communicating effectively, leading to diabetic cystopathy.
Read this : Hypertensive Retinopathy vs Diabetic Retinopathy
Why Diabetic Cystopathy Happens
The journey from a healthy bladder to diabetic cystopathy does not happen overnight. It is a slow process driven by a combination of factors.
Chronic high blood sugar is the primary culprit. When glucose levels remain high for years, it damages the tiny blood vessels that supply oxygen and nutrients to your nerves. Without proper blood flow, the autonomic nerves connected to your bladder begin to degrade and die.
At the same time, this nerve damage leads to detrusor muscle dysfunction. The detrusor is the main muscle of the bladder wall. When its nerve supply is cut off, the muscle becomes weak and sluggish.
Furthermore, high blood sugar causes urothelial changes. The urothelium is the protective inner lining of the urinary tract. Diabetes alters this lining, making the bladder tissue stiffer and more prone to dysfunction. This multifactorial pathophysiology makes diabetic cystopathy a complex condition to manage.
How Diabetes Affects the Bladder
To understand how diabetes damages the bladder, imagine the bladder as a highly sensitive, stretchy water balloon.
Normally, as the bladder fills with urine, it sends signals to the brain. When it is half-full, you feel the urge to go. When you reach the washroom, the bladder muscle squeezes tightly, emptying the balloon completely.
Diabetes disrupts this entire mechanism. First, it causes bladder sensation changes. The damaged nerves fail to tell the brain that the bladder is full. As a result, you might go hours without feeling the urge to urinate.
Because you are holding urine for so long, you experience a bladder capacity increase. The “balloon” overstretches. Over time, this extreme stretching ruins the elasticity of the muscle, leading to poor emptying. When you finally try to urinate, the muscle cannot squeeze hard enough.
This leaves a significant amount of urine behind in the bladder after you finish, which doctors call post-void residual urine.
Early vs Late-Stage Diabetic Cystopathy
Diabetic cystopathy is a progressive disease. The symptoms you experience will change dramatically as the condition advances.
In the early stages, patients often experience storage symptoms. The bladder nerves may become hyperactive before they fail, leading to sudden urges to urinate or frequent trips to the washroom. At this stage, the condition is often misdiagnosed as an overactive bladder.
In the late stages, the disease shifts from a storage problem to an emptying problem. The nerves become severely damaged, and the bladder muscle becomes floppy and weak.
This progression over time leads to mixed symptom patterns. A person might feel a sudden, desperate urge to urinate, but when they reach the toilet, they can only produce a weak, slow trickle of urine.
Common Symptoms of Diabetic Cystopathy
Because diabetic cystopathy develops slowly, many people adapt to their symptoms without realising something is wrong. Here is what to watch out for:
Decreased Bladder Sensation
You may notice that you can go for very long periods—sometimes 8 to 12 hours—without feeling the need to urinate. The normal pressure and fullness that signal a full bladder simply fade away.
Urinary Hesitancy
When you stand or sit at the toilet, the urine does not start flowing immediately. You may have to wait, focus, or even press on your lower stomach to get the stream started.
Weak Urine Stream
Instead of a strong, continuous flow of urine, the stream becomes very slow, weak, or dribbling. It may stop and start multiple times during a single washroom visit.
Feeling of Incomplete Emptying
Even after you have finished urinating and zipped up your trousers, you might feel a heavy sensation in your lower abdomen, as if you still need to go.
Increased Post-Void Residual Urine
This is a clinical sign where a large pool of urine remains trapped in your bladder after you urinate. While you cannot see this symptom, it is the root cause of many complications like infections.
Urinary Frequency and Urgency
Paradoxically, because the bladder is always partially full of leftover urine, it takes very little new urine to fill it to the brim again. This causes you to run to the washroom frequently, both day and night.
Overflow Incontinence or Leakage
When the bladder becomes massively overstretched and full of trapped urine, the pressure inside forces small amounts of urine to leak out. This often happens without any warning, especially when coughing or sneezing.
Recurrent Urinary Tract Infections
Urine that sits stagnant in the bladder is a perfect breeding ground for bacteria. People with diabetic cystopathy often suffer from urinary tract infections (UTIs) every few months.
Diabetic Cystopathy vs Overactive Bladder vs Urinary Retention
Because urinary symptoms can overlap, distinguishing between these conditions is vital for correct treatment.
Overactive bladder (OAB) is primarily a condition where the bladder muscle spasms suddenly, causing extreme urgency and frequent urination. The bladder usually empties well.
Urinary retention is the inability to empty the bladder completely, often caused by a physical blockage like an enlarged prostate in men.
Diabetic cystopathy is unique because it is a nerve issue that eventually causes chronic urinary retention. However, early on, the nerve irritation can mimic overactive bladder. This overlapping of symptoms is why confusion happens in clinics, and why a thorough medical evaluation is strictly required.
Who Is at Higher Risk of Diabetic Cystopathy?
Not everyone with diabetes will develop bladder problems. However, certain factors drastically increase your chances.
A long duration of diabetes is the biggest risk factor. People who have had diabetes for 10 years or more are at a much higher risk.
Poor glycaemic control plays a massive role. Patients with a consistently high HbA1c level suffer nerve damage at a much faster rate.
If you already have diabetic neuropathy (such as tingling, numbness, or pain in your feet), you are highly likely to develop bladder nerve damage as well. Older age also naturally weakens the bladder, compounding the effects of the disease. While it occurs in both types of diabetes, the type 1 vs type 2 context matters; Type 1 patients may develop it at a younger age due to a longer lifetime exposure to the disease.
Pathophysiology of Diabetic Cystopathy
To truly understand how to treat this condition, we must look at the pathophysiology—the biological mechanism of the disease.
Autonomic Neuropathy
High blood glucose leads to the accumulation of toxic byproducts that damage the myelin sheath (the protective coating around nerves). This demyelination slows down nerve signals, resulting in autonomic neuropathy that disconnects the bladder from the spinal cord.
Detrusor Underactivity
The detrusor is the smooth muscle of the bladder. Because it stops receiving regular electrical signals from the nerves, the muscle fibres start to shrink and weaken. This leads to detrusor underactivity, meaning the muscle cannot generate enough force to push out urine.
Bladder Wall and Urothelial Changes
Diabetes causes chronic oxidative stress and inflammation. This damages the urothelium, the innermost lining of the bladder. The bladder wall responds by depositing thick, stiff collagen fibres, making the organ rigid.
Impaired Bladder Contractility
Due to the nerve damage and the stiffened bladder wall, overall contractility is severely impaired. The bladder essentially becomes a passive, floppy bag rather than an active, squeezing pump.
Increased Bladder Capacity
Because the patient loses the sensation of fullness, the bladder holds more and more urine over time. A normal bladder holds about 400 to 500 millilitres. A diabetic bladder can stretch to hold over a litre, further destroying muscle tone.
Residual Urine and Secondary Complications
The ultimate result of this biological cascade is a high volume of residual urine. This stagnant fluid creates immense pressure inside the urinary tract and serves as a bacterial playground.
How Diabetic Cystopathy Is Diagnosed
If you report urinary issues, your doctor will begin a systematic diagnostic process.
First, they will take a detailed medical history and perform a symptom assessment. They will ask about your blood sugar levels, your washroom habits, and any history of UTIs. A physical exam will help rule out other issues like prostate enlargement or pelvic floor prolapse.
A crucial part of the diagnosis is the post-void residual measurement. After you urinate, the doctor uses a quick, painless ultrasound on your lower belly to see exactly how much urine is left inside your bladder.
Your doctor may also ask you to keep a bladder diary for a few days, writing down exactly how much you drink, how often you urinate, and if you experience any leaks.
Urodynamic Testing in Diabetic Cystopathy
For a definitive diagnosis, a specialist may order a urodynamic test. This is the gold standard for evaluating bladder function.
Why urodynamics matters is simple: it shows exactly how the bladder behaves while it fills and empties. The doctor places a very thin catheter into the bladder to slowly fill it with water, while pressure sensors record the bladder’s response.
Classic findings in diabetic cystopathy during this test include a delayed first sensation to void (you don’t feel the water going in), an abnormally increased bladder capacity, and impaired contractility (the muscle doesn’t squeeze when asked to empty).
When it is needed, urodynamics helps the doctor confirm that the problem is nerve-related and not a physical blockage.
Other Tests Doctors May Recommend
To ensure your entire urinary system is safe, your doctor will run a few extra checks.
A urine routine and culture test is mandatory to check for microscopic blood, excess sugar, or active bacterial infections. An ultrasound of the kidneys and bladder is done to ensure urine is not backing up into the kidneys.
Kidney function tests, such as a blood test for creatinine and eGFR, ensure your kidneys are filtering waste properly. In some cases, a cystoscopy may be performed. This involves passing a tiny camera into the bladder to look for stones, tumours, or structural damage. Finally, a general neurological assessment of your reflexes can confirm the presence of widespread neuropathy.
Complications of Diabetic Cystopathy
Ignoring diabetic cystopathy is highly dangerous. It is not just an inconvenience; it threatens your major organs.
The most immediate danger is chronic urinary retention. When urine sits in the bladder, it leads to recurrent UTIs. These infections are stubborn, hard to treat, and can easily travel up the ureters into the kidneys.
Severe bladder overdistension leads to overflow incontinence, which causes significant emotional distress and hygiene issues.
The most severe complication is kidney damage risk. If the bladder is constantly full, the high pressure forces urine to flow backwards toward the kidneys (a condition called hydronephrosis). Over time, this back-pressure destroys kidney tissue, leading to irreversible chronic kidney failure.
Treatment of Diabetic Cystopathy
The treatment of diabetic cystopathy is highly individualised. It depends on whether your symptoms are mild, moderate, or severe.
The primary treatment goals are to achieve symptom control, improve complete bladder emptying, and prevent life-threatening kidney complications. Treatment usually involves a combination of lifestyle changes, medications, and sometimes physical interventions.
Non-Medical Management
Before prescribing heavy medications, doctors usually start with behavioural and lifestyle therapies.
Better Blood Sugar Control
This is the cornerstone of treatment. While you cannot easily reverse existing nerve damage, maintaining strict blood sugar control stops the neuropathy from getting worse.
Timed Voiding / Scheduled Voiding
Because your bladder cannot tell you when it is full, you must use a clock. Doctors recommend timed voiding, which means going to the washroom strictly every 3 to 4 hours during the day, whether you feel the urge to urinate or not.
Double Voiding Technique
This is a simple but highly effective trick. When you go to the washroom, sit and urinate as much as you can. Then, wait for 2 to 3 minutes, relax your muscles, and try to urinate again. This helps push out the residual urine.
Fluid Timing and Bladder Habits
Spread your fluid intake evenly throughout the day. Avoid drinking large amounts of water or caffeine right before bedtime to reduce nighttime trips to the toilet.
Pelvic Floor Support if Needed
For some patients, working with a physiotherapist to strengthen the pelvic floor muscles can help manage leakage and improve minor emptying issues.
Medical Treatment Options
If lifestyle changes are not enough, your doctor will introduce medications tailored to your specific bladder problem.
Medicines for Storage Symptoms
If you are in the early stages and experiencing urgency or frequency, your doctor might prescribe antimuscarinics or beta-3 agonists. These medications help relax the bladder muscle, allowing it to hold urine more comfortably without spasming.
Medicines for Bladder Emptying Problems
If your main issue is urinary retention, medications like cholinergics (such as bethanechol) may be used to try and stimulate bladder contraction, though their success rate varies. Alpha-blockers are also commonly prescribed to relax the muscles at the neck of the bladder, making it easier for urine to flow out.
Infection Treatment if UTIs Are Present
If you have a high post-void residual volume, you will likely get infections. Doctors will prescribe targeted antibiotics based on your urine culture. In severe cases, a low-dose daily antibiotic may be used as a preventative measure.
Managing Contributing Constipation or Prostate Issues
Severe constipation can press against the bladder and worsen emptying problems. Treating constipation with high-fibre diets and laxatives is crucial. For men, treating an enlarged prostate simultaneously is required for good urine flow.
Catheter-Based Management in Severe Cases
When the bladder muscle completely fails (detrusor areflexia) and medications do not work, physical intervention is necessary to protect the kidneys.
The gold standard treatment is Intermittent Self-Catheterisation (ISC) or Clean Intermittent Catheterisation (CIC). This involves the patient gently inserting a thin, sterile, disposable tube (catheter) into their urethra to drain the urine, usually 3 to 4 times a day.
While the idea of catheter use often scares patients, it is incredibly safe, painless once learned, and life-changing. It completely empties the bladder, stops overflow incontinence, drastically reduces UTIs, and removes the dangerous back-pressure on the kidneys.
Diabetic Cystopathy in Men vs Women
The disease behaves slightly differently depending on gender anatomy.
In men, the symptom differences often overlap heavily with benign prostatic hyperplasia (BPH), or an enlarged prostate. Both cause a weak stream and hesitancy. A urologist must carefully evaluate a diabetic man to see if his retention is caused by a blocked prostate, a weak diabetic bladder, or a combination of both.
In women, diabetic cystopathy often presents alongside pelvic floor weakness. Because women have shorter urethras, they are naturally more prone to UTIs. When you add post-void residual urine to the mix, recurrent UTI and incontinence considerations become a major daily struggle that severely impacts their quality of life.
Prevention of Diabetic Cystopathy
The best way to manage diabetic cystopathy is to prevent it from developing in the first place.
Strict blood sugar control is your primary shield. Keep your HbA1c within the target range set by your endocrinologist. Managing your blood pressure and cholesterol also protects the micro-blood vessels feeding your nerves.
Neuropathy prevention requires a healthy lifestyle, regular exercise, and quitting smoking. Most importantly, practice early reporting of urinary symptoms. Do not wait until you are leaking urine to tell your doctor. Routine follow-up appointments should always include a quick conversation about your bladder habits.
When to See a Doctor
You should never accept bladder problems as a “normal” part of ageing or diabetes. Seek medical advice immediately if you experience:
- Difficulty passing urine or having to push hard to start the stream.
- Recurrent UTIs or burning during urination.
- Unexplained urine leakage or continually damp undergarments.
- A sensation of lower abdominal fullness or pain.
- Worsening urinary symptoms that wake you up multiple times a night.
Real-Life Scenario
Mr. Sharma, a 62-year-old retired bank manager from Delhi, had been living with Type 2 diabetes for 15 years. Over the last two years, he noticed his urine stream becoming very weak. He also realised he only needed to urinate twice a day, but he frequently suffered from sudden, embarrassing urine leaks when he coughed.
Assuming it was just an age-related prostate issue, he ignored it. However, he eventually developed a severe fever and back pain. Rushed to the hospital, doctors found a massive kidney infection caused by over a litre of stagnant urine trapped in his bladder.
Mr. Sharma was diagnosed with advanced diabetic cystopathy. His doctor started him on a strict regimen of timed voiding and taught him how to perform Clean Intermittent Catheterisation (CIC) twice a day. Within a month, Mr. Sharma’s kidney function recovered, his urinary leaks stopped entirely, and he finally felt in control of his life again.
Expert Contribution
Dr. Rajesh Khanna, a leading urologist specialising in neurogenic bladders, explains the urgency of awareness:
“Diabetic cystopathy is often called the ‘silent complication’ of diabetes. Because the primary symptom is a loss of sensation, patients simply do not feel the damage happening. They think having a ‘strong bladder’ that can hold urine for 10 hours is a good thing, when in reality, it is a sign of dying nerves. I strongly urge every physician treating diabetic patients to ask one simple question at every visit: ‘How is your urine flow?’ Early detection saves kidneys.”
Recommendations Grounded in Proven Research and Facts
The medical management of diabetic bladder dysfunction is grounded in solid clinical guidelines.
According to the American Urological Association (AUA) and the European Association of Urology (EAU), tight glycaemic control is the only proven method to delay the onset of diabetic neuropathy, including cystopathy.
Furthermore, extensive research confirms that for patients with severe retention and high post-void residual volumes, Clean Intermittent Catheterisation (CIC) is the safest and most effective treatment. Studies show that CIC significantly reduces the risk of upper urinary tract damage and severe renal failure compared to relying solely on medications or long-term indwelling catheters.
Frequently Asked Questions on Diabetic Cystopathy
How to treat diabetic cystopathy?
Treatment focuses on emptying the bladder completely. It includes scheduled voiding (urinating by the clock), double voiding, medications to help relax the bladder neck, and in severe cases, Clean Intermittent Catheterisation (CIC) to physically drain the trapped urine and prevent infections.
Is diabetic cystopathy reversible?
No, advanced diabetic cystopathy is generally not completely reversible because the nerve damage (neuropathy) that causes it is permanent. However, with strict blood sugar control and proper urological treatment, the symptoms can be highly managed, and further progression can be stopped.
What are the 5 best foods for diabetics?
While managing diabetes overall helps the bladder, the top 5 foods for general blood sugar control include: 1) Leafy greens (like spinach), 2) Whole grains (like oats and millets), 3) Fatty fish (rich in Omega-3), 4) Nuts and seeds (like almonds and chia seeds), and 5) Beans and lentils (high in fibre).
How to diagnose diabetic cystopathy?
Doctors diagnose it by taking a medical history, testing the urine for infections, and using a post-void residual (PVR) ultrasound to see how much urine is left in the bladder after you pee. A definitive diagnosis is often made using urodynamic testing, which measures bladder pressure and nerve sensation.
Can diabetic cystopathy cause kidney failure?
Yes. If diabetic cystopathy is left untreated, the bladder becomes dangerously overstretched. The high pressure forces stagnant urine to flow backwards up the ureters into the kidneys (hydronephrosis). Over time, this back-pressure and recurrent infections can destroy kidney tissue, leading to chronic kidney failure.
Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. Always consult your doctor or a qualified urologist for a proper diagnosis and treatment plan regarding bladder health and diabetes management.


